1902 Encyclopedia > Hospital
Hospital
HOSPITAL is derived from the Latin hospitalis (adj.), and this again from the noun hospes, a host or guest. The place in which a guest was received was in Latin hospitium (hence the French, hospice), but in course of time the adjective became used as a noun, and the words hospitalis, hospitale, and hospitalia were adopted in the same sense as hospitium, by dropping the nouns clomus, cubiculum, or cubicula. In this sense Vitruvius uses hospitalia to mean the chambers where guests were received. The English word hospital (often reduced to spited) comes from the old French hospital, now hôpital, of which Littré says that it was remade from the Latin many centuries ago, although originally hospitalis had given rise quite regularly to hostel, now hôtel. The three words, hôpital, hospice, and hôtel, although from the same source, are used now in very different meanings, the first being usually restricted to establishments for temporary occupation by the sick and hurt, for the purposes of medical and surgical treatment ; the second (hospice) to places for permanent occupation by the poor, the infirm, the incurable, or the insane ; and the last (hôtel) to dwellings, either public or private, for ordinary occupation. To the last, however, there is one exception, viz., when the term hôtel-Dieu (that is, hôtel de Dieu) is applied to the chief hospital or infirmary of a town or city. In English we have no equivalent to hospice, so that the word hospitcd has been, and is still, used in the double sense, viz., as a place for medical treatment, and also as a retreat or almshouse for the poor, the infirm, &c. On the other hand the word infirmary, which originally meant a place or room set apart in an establishment (such as a monastery) for the reception of the sick members, and also for those who were through age or infirmity incapacitated from work, is not infrequently employed in the same sense as hospital, namely, as a separate establishment for the treatment of the sick.
Although in ancient times there may have been places for the reception of strangers and travellers, it seems at least doubtful if there was anything of the nature of a charitable institution for the reception of the sick, such as existed after the introduction of Christianity. The Bethesda of Scripture (Aramaic, from  , a house, and , a house, and  , charity) was probably no more than a collection of mere sheds built round the pool to whose waters miraculous healing powers were attributed. Among the Greeks there seems little evidence of the existence of establishments for the sick ; xenon [Gk.], described by Plato as a place of shelter for travellers, is also explained as a nosokomeion [Gk.], or hospital, by Suidas ; but that lexicographer is a late writer (10th or 11th century A.D.), and the word nosokomeion [Gk.] itself does not appear to be earlier in use than the 4th century A.D. The word is used by St Jerome in the 4th century, and in the Code of Justinian in the 6th, from which it is possible Suidas may have got his definition, although xenodocheion [Gk.] is distinctly used by Justinian as a shelter for travellers, as indeed its name implies. Even for sick and wounded soldiers but little provision seems to have been made, although we do not know much of the valetudinarium, which appears to have existed in a Roman camp. That the Romans had a medical staff has been shown by the monuments discovered in Great Britain, and the subject has been carefully examined by the late Sir James Simpson (Transactions of the Society of Antiquaries of Scotland, Edinburgh Monthly Journal of Medicine, &c). Among the earliest hospitals on record are that said to have been founded by Valens in Caesarea 370-80 A.D., and the one built at Rome by Fabiola, a Roman lady and friend of St Jerome, although like most others of that and even later times both were probably almshouses as well. , charity) was probably no more than a collection of mere sheds built round the pool to whose waters miraculous healing powers were attributed. Among the Greeks there seems little evidence of the existence of establishments for the sick ; xenon [Gk.], described by Plato as a place of shelter for travellers, is also explained as a nosokomeion [Gk.], or hospital, by Suidas ; but that lexicographer is a late writer (10th or 11th century A.D.), and the word nosokomeion [Gk.] itself does not appear to be earlier in use than the 4th century A.D. The word is used by St Jerome in the 4th century, and in the Code of Justinian in the 6th, from which it is possible Suidas may have got his definition, although xenodocheion [Gk.] is distinctly used by Justinian as a shelter for travellers, as indeed its name implies. Even for sick and wounded soldiers but little provision seems to have been made, although we do not know much of the valetudinarium, which appears to have existed in a Roman camp. That the Romans had a medical staff has been shown by the monuments discovered in Great Britain, and the subject has been carefully examined by the late Sir James Simpson (Transactions of the Society of Antiquaries of Scotland, Edinburgh Monthly Journal of Medicine, &c). Among the earliest hospitals on record are that said to have been founded by Valens in Caesarea 370-80 A.D., and the one built at Rome by Fabiola, a Roman lady and friend of St Jerome, although like most others of that and even later times both were probably almshouses as well.
A physician visiting the sick in a hospital
(Source: German engraving from 1682)
The origin of our present hospitals must, however, be looked for in the monastic arrangements for the care of the sick and indigent. Every monastery had its infirmaria, managed by an infirmarius, in which not only were sick and convalescents treated, but also the aged, the blind, the weak, &c, were housed. [301-1] In course of time separate buildings were erected for the purpose, and special revenues, augmented from time to time by benefactions, appropriated for their maintenance. In numerous instances, however, the hospitals were converted into benefices by the priests, and the scandal had to be dealt with by the authority of general councils, which, like that of Vienne, forbade the practice. About the earliest distinct record of the building of a hospital in England is in the life of Lanfranc, archbishop of Canterbury, who in 1080 founded two, one for leprosy and one for ordinary diseases. The former is referred to in the Vie de St Thomas le Martyr, a work of the 12th century. The establishments for the sick remained in the hands of the clergy until the Reformation, when some of the monasteries and church property were appropriated and set apart for the use of the sick. Of those the most noted instances were St Bartholomew's in Smithfield, St Thomas's in the Borough, Bethlehem or Bedlam, Bridewell, and Christ's Hospital, which were long known as the "Five Royal Hospitals." St Bartholomew's was a priory, founded by Rahere, a minstrel, in 1102, and the ancient hospital chapel is still the parish church of St Bartholomew the Less. It was handed over to the citizens of London as a hospital in 1547 ; it escaped the fire of 1666, and was rebuilt in 1729. St Thomas's was founded by Richard, prior of Bermondsey, in 1213, surrendered in 1538, and purchased by the mayor and citizens of London in 1551, and opened for 260 sick. It was incorporated in 1553, rebuilt in 1693, added to in 1732, removed temporarily to Surrey Gardens in 1862, and finally transferred to Lambeth, its present site, in 1871. Bethlehem (or Bedlam) was a priory, founded by Simon Fitzmary, in 1247. In 1547 it was handed over by Henry VIII. for the reception of lunatics. It was rebuilt in 1676, and wings were added in 1733. The present building was constructed in 1810. Bridewell and Christ's Hospital early ceased to be receptacles for the sick. (For further information regarding charitable institutions see ENGLAND, vol. viii. p. 253.)

Appalling conditions in Bethlem (Bedlam) Hospital from the William Hogarth's A Rake's Progress.
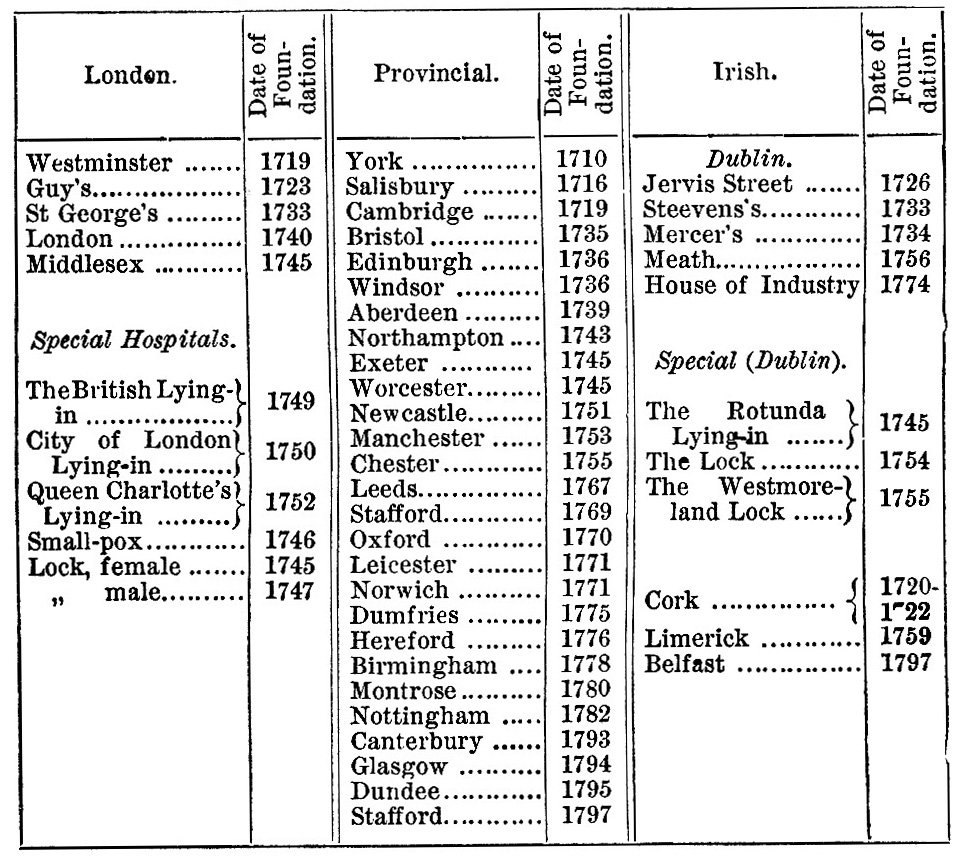
But the great movement in hospital building took place in the 18th century, and the following table from Dr Steele's paper, " On the mortality of Hospitals " (Howard prize essay for 1876), gives a list of the chief institutions founded during that period :—
During the present century the increase of hospitals has continued, seven general and many special having been founded in London alone. Dr Steele gives statistics of 27 metropolitan hospitals, having an aggregate of nearly 6000 beds, and receiving about 46,000 in-patients annually. This does not take into account the infirmaries attached to the workhouses or the metropolitan asylums hospitals. In addition to this probably from ten to twelve times the number of out-patients are treated in the course of the year.
Hospitals are usually divided into General and Special. In General Hospitals cases of all kinds are admitted in some, whilst in others certain classes are excluded. Thus cases of contagious zymotic disease are not admitted now in many instances, especially in London since the establishment of the metropolitan asylums, fever and small-pox hospitals. Lying-in cases, venereal cases, &c, are also frequently excluded.
Special Hospitals are of various kinds, such as lying-in hospitals, ophthalmic, lock (for venereal diseases), cancer, consumption, &c, besides fever and small-pox hospitals. At the end of the last and beginning of this century fever hospitals were generally called " houses of recovery," with a view of not alarming the people too much who had to resort to them. Special hospitals are also set apart for the treatment of diseases of children.
Besides the various civil hospitals there are also naval and military hospitals for the cure of sailors and soldiers.
Nightingale improving conditions in Scutari military hospital, Turkey, during the Crimean War
(Source: 1856 lithograph)
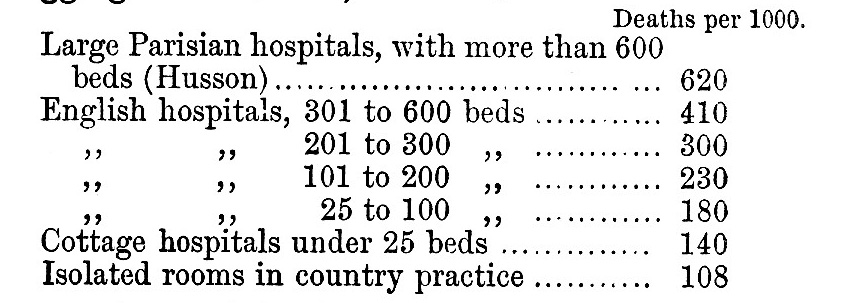
Although hospitals have been intended as a blessing and benefit to the poor, they have too often proved the reverse, on account of the ignorance, on the part of their administrators, of the true principles of health. So much was this the case formerly that it has been not infrequently debated whether hospitals are or are not gigantic evils; and even where it is admitted that they are of value in cases of actual disease, it is still doubtful if they are really of benefit in cases of confinement It may be of use to consider briefly the statistics of mortality at different times and in different places. It is very difficult to compare former death-rates with present or recent if we consider cases in bulk, because previous to the present century it was but little the custom to classify cases ; so that a preponderance of surgical cases might exist at one period and of medical at another, with a corresponding variation of the death-rate. Of course in some exceptional instances we can point to remarkable differences due to known causes of unhealthiness. Thus in the Hôtel Dieu of Paris, in the last century, a terrible mortality occurred, amounting to 1 in 4 1/2, or 220 per 1000 (Tenon) ;—and in the British hospitals at Scutari the mortality reached between 400 and 500 per 1000. In both of those cases there was inordinate crowding, such as is hardly likely to be met with again. But in dealing with ordinary hospitals there are so many modifying causes that the comparison, without careful analysis, may be misleading. Thus Dr Steele has shown that in the last century (1730-1800) the death-rate of St Thomas's was 86 per 1000, whilst that of Guy's was 119 ; but this, as he points out, may have arisen from the latter being looked upon as an asylum for incurables. In 1875 the death-rates of the general hospitals in London ranged from 72 per 1000 in the Royal Free to 127 in King's College ; in the Edinburgh Royal Infirmary it was 92, and in the Glasgow 118. But it is when we examine the mortality of special cases that the most instructive lessons are to be learned ; and the best for this purpose are surgical cases and lying-in cases. From these we gather that the mortality is pretty generally in the ratio of the size of the hospital and the consequent aggregation of patients, the crowding together of patients in the wards, the deficiency of ventilation, defective sewerage arrangements, and the want of constant attention to the details of cleanliness. Thus Sir James Simpson showed in his paper on " Hospitalism " the following statistics of mortality from amputations :—
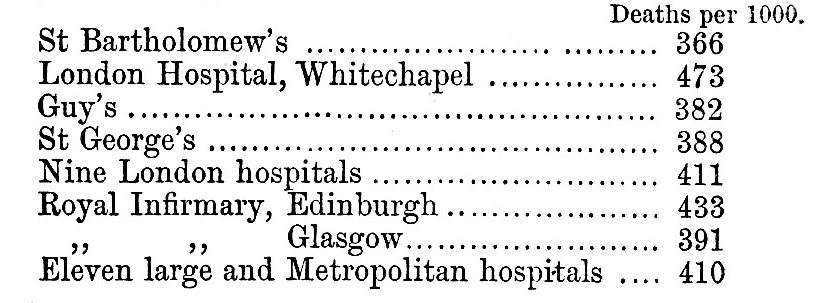
On the other hand, amputations in country practice give a death-rate of only 108 per 1000.

Entrance to Guy's Hospital, London, in 1820.
Comparing the results with the size of the hospital, that is, the aggregation of cases, we find:—
The question of lying-in cases is even more remarkable. Dr Lefort, having collected the statistics of 888,302 delivered in hospitals, and of 934,781 delivered at home, shows that in hospitals 35 per 1000 die, and at home 4 3/4.
Dr Steele gives the statistics of the four great lying-in hospitals of London, compared with the "extern-maternity" charities of Guy's, St Bartholomew's, and St Thomas's :—
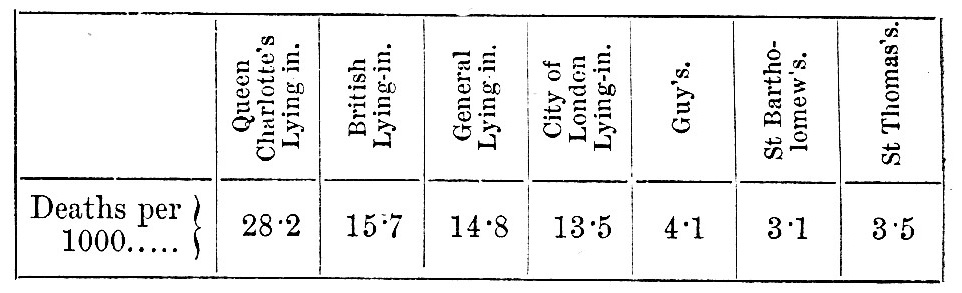
Baron Meydell, chief of the sanitary department of St Petersburg, has shown that in the largest lying-in hospital there, in which 2000 women are confined in a year, the death-rate is from 30 to 40 per 1000; in the second, in which about 1000 women per annum are received, only 25 die ; in the third, where 400 are received, only 20 die per 1000; in the small detached asylums of 2 or 3 beds, of which there are 11 in different parts of the city, giving accommodation to 1600 women per annum, or about 155 each, only 9 per 1000 die; whilst amongst those confined in their own homes, including the poorest and most wretched, only 5 per 1000 die (Rapport du Congres International d'Hygiene et de Sauvetage, Brussels, 1876, vol. i. p. 226). These numbers correspond with the observations above.
It can also be shown that outbreaks of disease are coincident with individual overcrowding, whether the hospital be large or small. Thus the terrible mortality of the Hotel-Dieu of Paris in the last century was due as much to actual overcrowding as to the enormous aggregation of patients. The extraordinary spectacle was to be seen there of two or three small-pox patients, or several surgical cases, or sometimes even four parturient women, lying in one bed. A large proportion of the beds were purposely made for four patients, and six were frequently crowded in. In the Salle St Charles and St Antoine there were 139 large beds (intended for four patients each, but often holding six), and 38 small beds for one patient each. Those beds were generally full, giving under ordinary conditions 558 patients, and in times of pressure 836. To this might be added the Salle St Roch, opening directly from and really forming part of the great ward ; this contained 35 large beds and 3 small,—normal number of patients 143, with a possible increase to 213. This gives a grand total of 701 patients as a normal amount, with a possible increase to 1049. There was thus collected in one enormous ward a larger number of patients than any hospital in England contained altogether, if we except the Royal Naval Hospital at Haslar. In addition, however, to the above inordinate number, there were in the three stories placed above this great ward 1926 patients, which number might be increased to 2596,—without reckoning the serving staff of the institution ; —or (including the wards on the Pont Double) a total in one block of building equal to 3418, which might be increased to 4320. The law forbade the hospital authorities to refuse admission to anyone, and in 1773 there were 5000 patients in the hospital, which occupied a space of little more than 3 English acres,—giving a total gross area of only 30 square feet per head. The gross area per bed of the modern Hôtel-Dieu is just ten times this amount, being 311 square feet, according to M. Toilet ; but even this is much too small, 100 square metres (1076 square feet) being the minimum proposed by Toilet, who estimates the general average per inhabitant of Paris at 430 square feet, whereas that of London is nearly double. We cannot point to any such overcrowding in England as that of the old Hôtel-Dieu, but in many cases there has been enough to produce very grave results. The ill effects are seen in outbreaks of erysipelas, hospital gangrene, and surgical fever among surgical cases, and in puerperal fever in lying-in cases,'—whilst in all communicable diseases the danger of spreading is greatly intensified. It was observed in 1877 in the General Lying-in Hospital, the year before it was closed for alterations, that when only two or three women were in a ward, puerperal disease rarely showed itself, but that when, in consequence of pressure of applications, five or six were put in, disease generally broke out. j Similar results have been observed elsewhere.
Another great cause of mortality has been inefficient ventilation. If we can scatter our sick population and give them individually plenty of space in their wards, we shall have done much,—but, if we do not also change the air sufficiently often we may still have evil results with all our I care. Formerly no arrangements were made for ventilation in hospitals, schools, barracks, churches, or indeed in any buildings whatsoever. An immense deal remains to be desired in this direction still, but in recent hospitals, at least, more or less efficient means have been introduced, whilst efforts have been made to improve the conditions of the old. The want of fresh air aggravates all diseases, increases the power of infection, retards the convalescence, and hastens the death of patients ; moreover, it lowers the tone of the healthy, and is the most potent of all agents in the propagation of phthisis or destructive lung disease. The labours of the Royal Commission of 1857, appointed to inquire into the health of the army, brought out in full relief the disastrous effects of want of proper ventilation in the sleeping rooms of our soldiers. It was there shown that the death-rate of Her Majesty's Foot Guards was more than 20 per 1000 per annum, 67 per cent, greater than the death-rate at the same ages in Manchester, our most unhealthy town, double the general death-rate of England, and nearly three times that of the most healthy country districts. As regards phthisis alone the death-rate was 10.8 per 1000 from 1830-1836, and 11.9 from 1837 to 1846, or an average of 11.4 per 1000 for the period, an amount more than the total mortality of the civil male population of England and Wales at the same ages. In the army generally the proportion was 7.86. Since the evil was recognized steps have been taken to remedy the conditions, particularly in the direction of giving more space in barrack-rooms, and securing a certain standard of air renewal. The results are seen in the present death-rate from phthisis, which is reduced to 2.5 per 1000, about one-third of the old, and not much above that of the best districts in England. It is still, however, too high, as a large number of men are invalided for disease who go to swell the returns of sickness and mortality in civil life. That this is mainly owing to defective air renewal is evident from the fact that in civil life starvation, crowding, and poverty are insufficient to produce the same evil results we have seen in our army,—because, in all likelihood, the very wretchedness of the dwellings of the poor has brought about an amount of involuntary air renewal, which has been their safeguard.
Defective arrangements for the removal of excreta have constituted another cause of mortality. Water closets opening directly out of wards, and sinks, waste-pipes, bath-pipes, &c, in direct communication with the sewers, have been the means of introducing sewer poison into hospitals, producing surgical and puerperal diseases, enteric fever, and diphtheria, and aggravating every other form of malady.
A want of constant attention to the details of cleanliness has been a fertile source of hospital disease. Dr B. W. Richardson has traced out in a very instructive way the remarkable immunity of the Jews from epidemic and other diseases, and has shown that their religious attention to the details of the periodic cleansing enjoined by the Mosaic law appears to he the main cause of this notable circumstance. An instructive instance of the importance of this point is recorded by Mr W. Cadge, surgeon of the Norwich Infirmary, which institution had long suffered from surgical diseases, such as erysipelas, pyaemia, and the like. These, it was supposed, were mainly due to the age and structural defects of the building, so that it was determined to pull it down and reconstruct it throughout. In the meantime a change of administration took place, and a new matron was introduced, who effected an entire alteration in the arrangements, and in particular insisted on an absolute and unremitting attention to every detail of cleanliness, both of building, clothing, bedding, and person. The result was an immediate cessation of the dreaded complications which had so vexed the hospital, and from that time there has been no return of them.
Faulty diet had also, doubtless, its influence on mortality, although its effects would be less easy to trace. One singular feature in the last century was the enormous allowance of beer given to patients in hospital,—from two to three pints being common, and the allowance sometimes reaching half a gallon per diem. The absence of fresh vegetables from the diet, not only of hospitals but also of the populace at large, probably introduced a scorbutic taint which may have had some part in aggravating or modifying disease.
Some influence must also be allowed to the indiscriminate mixture of cases. The evil of this, especially in the more or less crowded state of the older hospitals, was recognized even in the last century, and was referred to by Tenon among others. Although the danger is materially lessened when ample space per bed is allowed, it is still unadvisable, not to say unfair, to place contagious cases with other patients. The argument has been advanced that by distributing infectious cases there is less danger of concentration of poison than when they are congregated together by themselves. With proper hygienic precautions, however, this concentration may be minimized, whilst the isolation of such cases gives the greatest immunity to others.
This question of concentration has been pushed still further, so as to bear against the existence of all hospitals whatsoever, and so far as lying-in hospitals are concerned we have seen that the objections are well founded. But when we consider the subject in its various aspects it must be admitted that it would be difficult to do without hospitals in some form or another. It would hardly be possible to afford people the same advantages of treatment, attendance, nursing, and comforts at their own homes, although in some cases the system of home treatment might be advantageously substituted, as has been done for so many years with so much success in Edinburgh and other towns of Scotland on the dispensary system. Another most important aspect of the question is the necessity for hospitals as places of instruction for those entering the profession of medicine. Although it would be wrong to subordinate in any serious way the claims of patients of any class to the requirements of teaching, it must yet be admitted that the only sound way of learning medicine and surgery is by clinical or bedside instruction, and we may therefore reasonably demand that those who owe their treatment and care to public charity should be willing so far to contribute to the general welfare. Now it is clear that in dealing with large classes of students it would hardly be possible to convey proper clinical instruction except in a hospital. For this purpose the provincial hospitals ought to be more largely utilized, in addition to the metropolitan ; at present the resources of the former are to a great extent wasted for teaching purposes.
Assuming then the necessity for hospitals, there still remains the question of the kind of hospital that should be constructed or approved of. It is certainly open to doubt whether we should continue to build monumental hospitals, and not rather construct slighter buildings, which may be destroyed and rebuilt from time to time, thus both scattering patients over a wider area and lessening the risk from long accumulation of infective material. This latter has been named the cottage or hut system of construction. The difficulties attending it are chiefly connected with original expense of site and with the current expenses of nursing and administration. On the other hand, it may be urged with some reason that with correct hygienic management there is no reason why a large hospital should not be kept in a healthy condition.
We may now consider the principles of hospital construction.
1. Locality and Site.—Hospitals are required for the use of the community in a certain locality, and to he of use they must be within reach of the centre of population. Formerly the greater difficulty of locomotion made it necessary that they should be actually in the midst of towns and cities, and to some extent this continues to prevail. It is at least doubtful if this be the best plan. Fresh and pure air being a prime necessity, as well as a considerable amount of space of actual area in proportion to population, it would certainly appear to be better to place hospitals as much in the outskirts as is consistent with considerations of usefulness and convenience. In short, the best site would be open fields; but, if that be impracticable, a large space—a "sanitary zone," as it is called by Toilets—should be kept permanently free between them and surrounding buildings, certainly never less than double the height of the highest building. The difference between the expense of purchase of land in a town and in the environs is generally considerable ;—and this is therefore an additional reason for choosing a suburban locality. Even with existing hospitals it would be in most cases pecuniarily advantageous to dispose of the present building and site and retain only a receiving house in the town. St Thomas's in London, the Hôtel-Dieu in Paris, and the Royal Infirmary in Manchester are all good examples where this might have been carried out. In none, however, has this been done, the first two having been rebuilt, at enormous outlay, in the cities as before, although not exactly in the same locality, while the last is still retained with a few structural alterations. In Edinburgh, on the other hand, an open space of a much more favourable character has been obtained, which, although within the limits of the city, is almost rural in character.
As regards the actual site itself, where circumstances admit of choice, a dry gravelly or sandy soil should be selected, in a position where the ground water is low and but little subject to fluctuations of level, and where the means of drainage are capable of being effectually carried out. There should also be a cheerful sunny aspect, and some protection from the coldest winds.
2. Form of Building.—Á form of building must be selected which answers the following conditions:—(a) the freest possible circulation of air round each ward, with no cul-de-sac or enclosed spaces where air can stagnate; (b) free play of sunlight upon each ward during at least some portion of the day; (c) the possibility of isolating any ward, or group of wards, effectually, in case of infectious disease breaking out; (d) the possibility of ventilating every ward independently of any other part of the establishment. Those conditions can only be fulfilled by one system, viz., a congeries of houses or pavilions, more or less connected with each other by covered ways, so as to facilitate convenient and economical administration. The older plans of huge blocks of building, arranged in squares or rectangles, enclosing spaces without free circulation of air, are obviously objectionable. Even when arranged in single lines or crosses they are not desirable, as the wards either communicate with each other or with common passages or corridors, rendering separation impossible. On this point it may be remarked that some of the buildings of the last century were more wisely constructed than many of those in the first half of the present, and that the older buildings have been from time to time spoilt by ignorant additions made in later times. The question next arises —Is it better to have pavilions of two or more stories high, or to have single-storied huts or cottages, scattered more widely ? Where land is expensive the former plan is of course more economical, but where land is easily got the latter ought to be adopted. The pavilions may be arranged in various ways: they may be joined at one end by a corridor, or may be divided by a central corridor at right angles to them, &c. In fact, the plan is very elastic, and adapts itself to almost any circumstances. A certain distance, not less than twice the height of the pavilions, ought to be preserved between them. By this means free circulation of air and plenty of light are secured, whilst separation or isolation may be at once accomplished if required.
3. Foundations, Building Materials, etc.—It is of the first consequence that a hospital should be dry; therefore the foundation and walls ought to be constructed so as to prevent the inroads of damp. An impervious foundation has the further advantage of preventing emanations from the soil rising up in consequence of the suction force produced by the higher temperature of the internal atmosphere of the building itself. There should be free ventilation in the basement, and the raising of the wdiole on arches is a good plan, now generally carried out in hot climates. If the pavilions are two or more stories high it is advisable to use fire-proof material as much as possible, but single-storied huts may be of wood. In any case effectual means of excluding damp must be employed. The interiors of wards ought to be rendered as non-absorbent as possible, by being covered with impervious coatings, such as glazed tiles (parian, though much used, is apt to crack), silicate paint, soluble glass, or the like. The ceilings ought to be treated in the same way as the walls, or, perhaps better still, they might be made like the deck of a ship, without any lath and plaster, so as to have nothing but the floor itself between room and room. For the floors themselves various materials have been suggested: in France there is a preference for flags (dalles), but in England wood is more liked; and indeed hard well-fitting wood, such as teak, oak, or pitch-pine, leaves nothing to be desired. The surface should be waxed and polished or varnished. Even deal floors can be rendered non-absorbent by waxing, by impregnating them with solid paraffin as recommended by Dr Langstaff, or by painting with soluble glass as suggested by Dr Luther of Philadelphia.
4. Shape and Arrangement of Wards. —It is now generally agreed that wards should have windows on at least two opposite sides, and three main shapes have been proposed, viz., (a) long wards with windows down each side, and (generally) one at the further end; (b) wards nearly square, with windows on three sides; and (c) circular wards, with windows all round. The first (a) is the form usually adopted in pavilions; (b) is recommended by Dr Folsom (Plans for the Johns Hopkins Hospital) ; and (c) has been suggested by Mr John Marshall, F. K. S. (Nat. Assoc. for Promotion of Social Science, 1878). Of these (6) seems the least to be commended, and (c) has not yet been tried in practice; we may therefore confine our attention to the long or oblong wards. The length is to be determined chiefly by the number of patients to be accommodated, but the breadth admits of less variation. Each bed should be a little distance, say from 8 inches to 1 foot from the wall, and each bed may be reckoned as 6 1/2 feet long ; this gives 7 1/2 feet on each side. Between the ends of the beds about 10 feet space is necessary, so that 25 or 26 feet of total breadth may be taken as a favourable width. The wards of the Herbert Hospital are 26 feet; but some exceed this, as, for instance, St Thomas's, London, and the New Eoyal Infirmary, Edinburgh, 28 ; New Hotel-Dieu, 29; and Lariboisiere, 30. There seems no necessity for exceeding 26, but if the breadth be greater there ought to be more window-space,— the great difficulty being to get a wdde space thoroughly ventilated. There ought to be only two rows of beds, one down each wall, with if possible a window to each bed, and never less than one to every two beds.
5. Ventilation, Warming, and Lighting.—For ventilation two things are required,—sufficient space and sufficiently frequent change or renewal of air. As regards space, this must be considered with reference both to total space and to lateral or floor space. Unless a minimum of floor space be laid down, we shall always be in danger of overcrowding, for cubic space may be supplied vertically with little or no advantage to the occupier. If we allow a minimum distance of 4 feet between the beds and 10 feet between the ends of the beds, this gives 100 square feet of space per bed ; less than this is undesirable. In severe surgical cases, fever cases, and the like, a much larger space is required ; and in the Edinburgh New Infirmary 150 square feet is allowed. Cubic space must be regulated by the means of ventilation ; we can rarely change the air oftener than three times an hour, and therefore the space ought to be at least one-third of the hourly supply. This ought not to be less than 4000 cubic feet per bed, even in ordinary cases of sickness,— and the third of that is 1333 cubic feet of space. "With 100 square feet of floor space a ward of 13 1/2 feet high would supply this amount, and there is but little to be gained by raising the ceiling higher,— indeed, 12 feet is practically enough. The experiments of Drs Cowles and Wood of Boston (see Report of State Board of Health of Massachusetts for 1879) show that above 12 feet there is little or no movement in the air except towards the outlet ventilator; the space above is therefore of little value as ventilation space. Additional height adds also to the cost of construction, increases the expense of warming, makes cleaning more difficult, and to some extent hampers ventilation. Whatever be the height of wards, the windows must reach to the ceiling, or there must be ventilators in the ceiling or at the top of the side walls. If this be not arranged for a mass of foul air is apt to stagnate near the ceiling, and sooner or later to be driven down upon the inmates. The reasons for a large and constant renewal of air are of course the immediate removal and dilution of the organic matter given off by the inmates ; and, as this is greater in quantity and more offensive and dangerous in sickness than in health, the change of air in the former case must be greater than in the latter. Hence in serious cases an amount of air practically unlimited is desirable,—the aim of true ventilation being to approach as near as possible to the condition of pure ex-ternal air. Without going too much into details, a few general rules may be laid down :—(1) Fresh air ought if possible to be brought in at the lowest part of the ward, warmed if necessary; (2) foul air ought to be taken out at the highest part of the ward ; (3) fresh air should reach each patient without passing over the bed of any other ; (4) the vitiated air should be removed from each patient without passing over the bed of any other ; (5) 4000 cubic feet of fresh air per head per hour should be the minimum in ordinary cases of sickness, to be increased without limit in severer cases ; (6) the air should move in no part of a ward at a greater rate than 1 1/2 feet per second, except at the point of entry, where it should not exceed 5 feet per second, and at the outlet, where the rate may be somewhat higher ; about 64 square inches of inlet and outlet sectional area ought to be supplied per head as a minimum ; (7) every opportunity ought to be taken of freely flushing the wards with air, by means of open windows, when this can be done with safety.
Warming is a question of great importance in most climates, especially in such a climate as ours, where every system of ventilation must involve either the warming of some portion of the incoming air, or the contriving its delivery without too great lowering of temperature ; at the same time it cannot be too strongly insisted upon that the tendency is too much in the direction of allowing warmth to supersede freshness of air. There are very few cases of disease (if any) that are not more injured by foul air than by low temperature ; and in the zymotic diseases, such as typhus, enteric fever, small-pox, &c, satisfactory results have been obtained even in winter weather by almost open-air treatment. At the same time a reasonable warmth is desirable on all grounds if it can be obtained without sacrificing purity of atmosphere. For all practical purposes 60° to 63° F. is quite sufficient, and surgical and lying-in cases do well in lower temperatures. Various plans of warming have been recommended, but probably a combination is the best. It is unadvisable to do away altogether with radiant heat, although it is not always possible to supply sufficient warmth with open fire-places alone. A portion of the air may be warmed by being passed over a heating apparatus before it enters the ward, by having an air chamber round the fire-place or stove, or by the use of hot-water pipes in the ward itself. In each case, however, the air must be supplied independently to each ward, so that no general system of ventilation is applicable.
The lighting of wards at night wull be most conveniently done by means of gas, in the form of a jet over each bed, with a special ventilator to carry off combustion products, as in the Edinburgh New Infirmary.
6. Furniture of Wards.—This should be simple, clean, and non-absorbent ; the bedsteads of iron, mattresses hair, laid on spring bottoms without sacking. No curtains should be permitted.
7. Water. —The water-supply ought to be on the constant system, and plentiful ; 50 gallons per head per diem may be taken as a fair minimum estimate.
8. Closets, Baths, &e.—The closets ought to be of the simplest construction, the pans of earthenware all in one piece, the flushing arrangements moved by opening the door,—the supply of water ample. Each ward should have its own closets, lavatories, &c., built in small annexes, with a cross-ventilated vestibule separating them from the ward. All the pipes should be disconnected from the drains, the closets by intercepting traps, the sink and waste pipes by being made to pour their contents over trapped gratings. The soil pipes should be ventilated, and placed outside the walls, protected as may be necessary from frost. Each ward should have a movable bath which can be wheeled to the patient's bedside.
9. Each ward should have attached to it a room for the nurse from which she can look into the ward, a small kitchen for any special cooking that may be required, a room for the physician or surgeon, and generally a room with one or two separate beds. No cooking should be done in the wards, nor ought washing, airing, or drying of linen to be allowed there.
10. Nursing.—The arrangements for nursing the sick have greatly improved in recent times, although controversy still goes on as to the best method of carrying it out. In arranging for the nursing in a hospital both efficiency and economy have to be considered. Miss Nightingale recommends large wards of 32 beds each, as at the Herbert Hospital, on the ground that one head-nurse is sufficient for such a number by day and one nurse by night. In the Edinburgh New Infirmary the wards are not so large, the medical being arranged for 21, and the surgical for 14 patients. Circumstances must to a large extent determine the arrangement, but it seems desirable on the whole that the work of a nurse should be confined to a single ward at a time if possible. The duties of nurses ought also to be distinctly confined to attendance on the sick, and no menial work, such as scrubbing floors and the like, should be demanded of them ; a proper stall' of servants ought to be employed for such purposes. It is also desirable that a separate pavilion for lodging the nurses should be set apart, and that fair and reasonable time for rest and recreation should be allowed. Some discussion has taken place as to the advisability of placing the nursing of a hospital in the hands of a sisterhood or separate corporation. It will, however, be admitted that the best plan is for the nursing staff of each hospital to be special and under one head within the establishment itself, even although it may be connected with some main institution outside. The nursing must of course be carried on in accordance with the directions and treatment of the physicians and surgeons.
11. The kitchen, laundry, dispensary, and other offices must be in a separate pavilion or pavilions, away from the wards, but within convenient access.
12. A separate pavilion for isolation of infectious cases is desirable. This may be a wooden hut, or in some cases even a tent ; either is probably preferable to a permanent block of building.
13. A Disinfecting Chamber ought to be provided, where heat can be applied to clothes and bedding, for the destruction both of vermin and of the germs of disease. It is advisable to expose all bedding and clothing to its influence after each occasion of wear. Although this may entail additional expense from deterioration of fabric, it is worth the outlay to secure immunity from disease. This plan is rigidly followed at the Royal South Hants Infirmary at Southampton.
14. It is of great importance that the wards should be periodically emptied, and kept unoccupied for not less than one month in each year, and longer if possible. During such period thorough cleansing and flushing with air could be carried out, so as to prevent any continuous deposit of organic matter.
Up to quite lately hospital accommodation was confined to the larger towns, but the desirability of having it more accessible in smaller towns and villages has made itself more and more felt. Accordingly in many places cottage hospitals have been established with advantage. One great advantage of the pavilion system is that the principles of its construction and arrangements are equally applicable to large and small establishments, so that we may either look upon a large hospital as an extension of a cottage hospital, or upon a small one as a section of a pavilion one. The importance of increased accommodation for the reception of infectious cases is now very generally acknowledged, as shown not only by the establishment of the Metropolitan Asylums Hospitals, but also of others in various parts of the country. In some instances they have apparently been the means of arresting the spread of disease and protecting the locality from epidemics.
Paying Hospitals, Pay-Wards, Provident Dispensaries.— The general object for which hospitals have been established may be stated to be the gratuitous medical and surgical treatment of the indigent sick. Many abuses have, however, crept in, and large numbers of persons yearly receive medical treatment gratuitously who are quite able to pay for it. The numbers have been stated at one in four in London and one in two in Liverpool of the entire population. To obviate this evil the establishment of paying institutions has been much recommended. There is a large class above the very poor who are but ill able to afford the most skilled attendance and nursing at their own homes, which in most cases do not supply the accommodation necessary for sickness. It is not desirable, nor is it always their own wish, that those persons should be objects of : charity, and the establishment of hospitals and dispensaries at which they could contribute something towards the expense of their treatment and attendance would meet the difficulty to some extent. Numerous arrangements of the kind are to be found on the continent of Europe, in America, and in the British colonies. Attempts have recently been made to introduce the system into England, and it is highly desirable that it should be accomplished, if it can be done with fairness to all concerned.
Administration.—In the civil hospitals of Britain this | is usually carried on by a body of governors, who are either specially appointed or are benefactors of the institution. From them an executive committee is chosen, or the executive power may be vested in a single official, often the treasurer. A secretary or superintendent is usually charged with the financial and general management of the affairs of the hospital, whilst an apothecary superintends the pharmaceutic department. The treatment of the sick is of course entirely in the hands of the physicians and surgeons, whose appointments are for the most part honorary, in the sense of being unpaid, and under whom resident medical officers act. The medical staff ought always to be represented on the governing body as a means of preventing unnecessary friction. The appointment seems desirable in every hospital of a sanitary officer, whose duty it should be to watch and supervise the carrying out of every detail of ventilation, warming, cleanliness, disinfection, &c.
On the Continent hospitals are more directly under state control, and their arrangement is therefore considerably modified.
Naval and Military Hospitals.—These are provided in all civilized countries for the care of the sailors and soldiers of the state. The two great English hospitals of Greenwich and Chelsea were founded as asylums for disabled and superannuated sailors and soldiers, but the former is now given up for that purpose, although a part is appropriated as a hospital for sick merchant seamen of all nations. The chief naval hospitals are those of Haslar, Plymouth, and Chatham. Haslar is the largest hospital in the country, having been originally intended for 2000 sick, and even now, with increased allowance of space per bed, accommodating 1500 patients. There are also hospitals in most of the principal naval stations abroad, such as Malta, Jamaica, Halifax, Hong-Kong, &c. The principal military hospitals are the Royal Victoria Hospital at Netley (the invaliding hospital of the army and the locality of the army medical school), the Herbert Hospital at Woolwich, the Cambridge Hospital at Aldershott, and numerous others at the principal stations. The cubic space allotted by regulation is 1200 cubic feet at home and 1500 to 2000 cubic feet in the tropics per bed. Formerly every regiment of cavalry and infantry and each battery or troop of artillery had its' own hospital, but this plan is now given up, and station hospitals with a fixed staff are being arranged at the chief centres of military districts. In both the army and the navy the regulations place the administration and command of hospitals in the hands of the respective medical departments; in the army this is as yet only partially carried out, but it has been accomplished in the navy with the advantage of both efficiency and economy. In time of war general hospitals are established at the base of operations, whilst field hospitals move with the troops as the campaign progresses.
In France there have long been hospitals established for the navy, such as those at Rochefort, Toulon, Brest, &c, as well as schools of instruction for medical officers. The chief military hospital is the Val de Grâce at Paris, formerly a convent ; it is there that the medical school for the army is located. Large hospitals are also established in all the great stations. Great attention to military hospitals is also paid in Germany, Austria, and other countries of Europe. In most of them the administration is in the hands of the medical department, except in France, where the intendance still holds the reins, much to the disadvantage of efficiency and good working.
In the United States of America the army is small and chiefly employed on frontier duties, so that the hospitals are all what are called post hospitals, and as a rule are wooden huts or temporary structures, built to last ten years, and to hold 12 to 24 beds. There are, however, two permanent hospitals, one for cadets at West Point, and the other, the Barnes Hospital, at the Soldier's Home near Washington. All the arrangements are under the army medical department. The navy and the mercantile marine were long amalgamated in America, so far as hosrùtal arrangements went. The Marine Hospital Service was formed in 1798, and the navy was not separated from it until 1811, although it was not for some years after that special naval hospitals were built. In connexion with the marine hospital service, hospitals have been established at a great number of ports, both sea, river, and lake. Up to 1870 each of these hospitals had its own organization, but since that time a regular service has been established under a supervising surgeon-general. A tax of 40 cents a month is levied for the service upon all seamen or members whatsoever of a ship's company. One of the finest hospitals is the Mercantile Marine Hospital at Chicago, a pavilion building of several stories, and of considerable architectural pretensions. But in America, as in Europe, the tendency has latterly been to abandon such monumental hospitals, and to construct single-storied pavilions on the hut or " barrack " principle,—the word barrack being employed in this sense as equivalent to the French baraque, a wooden hut. Accordingly the new marine hospital at San Francisco has been thus constructed, three one-storied pavilions of Californian redwood radiating from the outside of a curved corridor, from the ends and inner centre of which project the administrative blocks. The cost is about £120 ($600) per bed, whereas the average cost of the older ones was fully seven times that amount, with the drawback that in course of time they became extremely unhealthy, and showed all the evils of hospitalism.
A brief notice may be added here of the history of hospital construction in recent times, particularly with reference to the pavilion system. It is to France that we must look for the commencement of that system, although it has been carried out with even greater success in other countries. Its origin may be traced to the discussions which arose from time to time as to the advisability of reconstructing the Hôtel-Dieu at Paris. So long ago as the 17th century, Desgodets, architect to Louis XIV., presented apian for reconstructing the hospital in "rayons." But it was after the fire that took place in 1772 that the question was taken up with real interest. In 1773 it was proposed to transfer the hospital to the plain of Grenelle, and in 1774 M. Petit proposed a radiating building of four stories at the base of the hill of Belleville (probably at no great distance from the existing hospital of Ménilmontant). M. le Roi presented a plan for a hospital at Chaillot, consisting of long single-story pavilions, arranged alternately, with the roof open at intervals,—each patient to be screened off by partitions. Finally, the committee of the Académie des Sciences reported favourably in 1788 on a proposal of M. Poyet's to construct a hospital on the Ile des Cygnes (between Grenelle and Passy), consisting of isolated pavilions radiating from a central rotunda, the hospital to hold 5000 patients,—each pavilion to be 115 feet long, by 24 broad and 14 to 15 high, to contain 34 to 36 patients, and to have windows to the ceiling. These proportions would give 77 to 80 square feet of floor space, 6 1/2 to 6 3/4 feet of wall space, and 1080 to 1200 cubic feet of total space, an immense advance upon then existing arrangements. The Revolution put a stop to those projects, and half a century elapsed before a pavilion building, as now understood, was actually constructed. Curiously enough, revolution again stepped in to arrest the movement, for the first building of the kind, the Hôpital Louis-Philippe, was begun in the last years of that monarch's reign, and suspended in consequence of the revolution of February 1848. Some years later, in 1854, it was completed and renamed Lariboisière, from the name of the benefactress whose munificence helped to bring it to a successful conclusion. The building is oblong, enclosing a space in the centre, the front (south end) containing the administration, and the opposite (north) end the chapel, kitchens, &c. From the two sides the pavilion wards jut out. The building is on the whole not a good one ; the distance between the pavilions is only half what is required, and the wards are frequently overcrowded. Unfortunately most of the defects, with some additional ones, have been reproduced in the new Hôtel-Dieu. The new hospital at Ménilmontant, in the north-east of Paris, is also a pavilion one, differing somewhat in detail, but of great size, each pavilion having numerous stories. The military hospital at Vincennes is a good specimen of modern construction. A small experimental pavilion, built on the suggestions of Dr Tarnier in the garden of the Maternité in Paris, merits notice. It consists of two stories, each containing four wards for one parturient woman each. The kitchen, office, &c., are in the centre, but the only access to each ward is by the verandah direct from the open air. The walls, floors, and ceilings are non-absorbent, aud there is a space of 56 cubic metres, or nearly 2000 cubic feet for each inmate. The chief objection is that there are no means of ventilation except by the door or window ;— otherwise the plan is excellent. This plan of making each ward open directly from the open air was proposed by the late Sir James Simpson, as a means of improving the sanitary state of existing old. hospitals. The plans of M. Toilet ought not to be passed unnoticed. In addition to the ordinary principles of pavilion construction, he insists upon the ogival or Gothic form of architecture, which he thinks was adopted in the Middle Ages as much for sanitary as for architectural reasons.
Florence Nightingale's book, Notes On Nursing
In England the question of hospital improvement slept until the disasters at Scutari, in 1854-55, roused the attention of the Government and the public to the necessities of the case, and the report of the Army Sanitary Commission and of the Barrack and Hospital Committee, and Miss Nightingale's Notes on Hospitals, led the way in advocating hospital reform. Unfortunately just before this movement the plans of Netley Hospital were made, and the building begun on the corridor system. Efforts were made to arrest i ts progress, but unhappily without effect, and the country which has led the van in sanitary science has as its chief military hospital a building far from satisfactory. The first pavilion hospital in England was the Blackburn Infirmary, built rather more than twenty years ago. The pavilions are there at right angles to a centre corridor, and are alternate ; a similar arrangement is followed out at the Children's Hospital at Pendlebury, near Manchester. St Thomas's at Westminster Bridge consists of a row of parallel pavilions united by a corridor at one end. A plan practically identical was proposed for a new hospital at Valetta (Malta), but this building, though frequently referred to in books, has never been constructed. The Herbert Hospital at Woolwich consists of parallel pavilions jutting out from the sides of a centre corridor at right angles ; although it is now nearly twenty years old, it is still one of the best examples of a pavilion hospital. The latest pavilion hospital is the New Royal Infirmary at Edinburgh, to : which reference has already been made. Every care seems to have been bestowed on its construction and arrangement ; the space allowed per head is ample and the site excellent.
In Germany the Friedrichshain Hospital at Berlin is one of the best specimens of a pavilion building. The pavilions are 160 feet apart, six two-storied and four one-storied, with isolation wards and the necessary administrative buildings. The hut hospital erected during the late war at Tempelhof near the same city was a good example of how the pavilion system may be indefinitely extended, the huts being placed in échelon in wide zigzag lines.
In America great attention has been paid to the question of hospitals, especially since its importance was so roughly thrust upon the country's notice in the great civil war of 1861-64. During that time numerous plans were tried, and among others the old plan of Petit, Poyet, &c., namely, radiating pavilions from a circular or oval centre, which contained the offices and administration. This plan was found not to be a good one, as it interfered with both lighting and ventilation. The earliest American hospital of any size was the Pennsylvanian Hospital of Philadelphia, which was begun in 1755, under the auspices of Dr Thomas Bond and Benjamin Franklin, and finished in 1805. It was also in Philadelphia that the first pavilion hospital of a permanent character was erected, the corner stone being laid in 1860 ; in it the pavilions are parallel, two stories besides basement and attics. The space allowed is ample, but the wards are too wide, nearly 31 feet. In New York there is a large amount of hospital accommodation—about 6000 beds, or about 1 in 1500 of the population. The New York Hospital new pavilions give 112 square feet of floor space and 1800 cubic feet of total space. The Roosevelt Hospital has somewhat the same dimensions, but with a much greater space for surgical patients. One peculiarity of arrangement in that building is that the closets are not at the end of the wards as usual, but in the centre, grouped round a central shaft which extends through all the stories, cellar and basement. In this the water and steam pipes are placed, as also the foul linen shafts ; the closets are cleaned by a steam jet. This plan does not seem very commendable. The Massachusetts General Hospital at Boston is the oldest in America, except the Pennsylvania Hospital. Since 1872 four new pavilions have been built on peculiar plans : two are square, one containing one large ward for 20 patients, and the other divided into small rooms of 2 beds each, giving each about 97 feet of floor space and 1500 to 1850 feet of total space ; the other two are oblong, divided into rows of single rooms, with a dividing corridor, something like an arrangement of prison cells. The floor space is about the same, with less height. The Johns Hopkins Hospital at Baltimore will be memorable for the care bestowed upon the consideration of its plans. The one finally adopted is on the pavilion principle, scattered over a wdde space of ground.
Bibliography.—Beckmann, History of Inventions (for ancient history of hospitals); Rapport des Commissionaires chargés par l'Académie de l'examen du projet d'un nouvel Hôtel-Dieu. Paris, 1786; Tenon, Mémoire sur les Hôpitaux, Paris, 1788 and 1810; Ibertl, Observations générales sur les Hôpitaux, 1788; Howard, An Account of Prisons and Lazzarettos in Europe, 1789 and 1791; Blizard, Suggestions for the Improvement of Hospitals, 1790; Pringle, Diseases of Armies, 1764; Brocklesby, Medical and Economical Observations, 1758-03; Blane, Médico-Chirurgical Transactions, vol. iv ; Jackson, Management of Hospitals, 1803; Ballingall, Observations on the Site and Construction of Hospitals, Edin., 1851 ; Roberton, Papers on Defects of Construction and Ventilation of Hospitals, Manchester, 1856-63: Parkes, Renkioi Hospital in the Dardanelles. London, 1857 ; Oppert, Die Einrichtung von Krankenhäusern, Berlin, 1859, and Hospitals, Infirmaries, and Dispensaries, London, 1807; Aitken, "On Site and Construction of Hospitals," Brit. and For. Med. Chir. Review, 1860; Report of the Royal Commission on the Health of the Army, 1857; Report of the Barrack and Hospital Committee, 1861; Report of the Barrack and Hospital Committee on Mediterranean Stations, 1863; Husson. Étude sur les Hôpitaux, 1862 ; Trélat, Étude critique sur la reconstruction de l'Hôtel-Dieu, 1863, and Des Hôpitaux, 1866; Nightingale, Notes on Hospitals; Galton, The Herbert Hospital, Woolwich, 1865, and Construction of Hospitals, Leeds, 1869; Report of Committee on Cubic Space in Metr. Workhouse Infirmaries, 1867 ; Waring, Cottage Hospitals, London, 1867; Parkes, Manual of Practical Hygiene, 5th edition, 1878; Swete, Handy Book of Cottage Hospitals, 1869; Nightingale, Notes on Lying-in Institutions, 1871; Simpson, Hospitalism, 1872; Beekman, Centenary Address, New York Hospital, 1871; Eilensen, Hospitalism, 1874; Buchanan, English Hospitals in their Sanitary Aspect, 1875; Plans for the Johns Hopkins Hospital, Baltimore, 1875; F. de Chaumont, "On Ventilation and Cubic Space," Lancet, 1866, and Edin. Med. Journ., 1867, " The Theory of Ventilation," Proc. Roy Soc., 1875-76, three Reports on St Mary's Hospital, Paddington, 1875, Reports on the Herbert and Hilsea Hospitals, Army Med. Reports, 1864, and Report on the Norwich Infirmary, 1878; Morin, Manuel du Chauffage et de la Ventilation, Paris, 1869; Wylie, Hospitals, their History, Origin, and Construction, New York, 1877; Burdett, The Cottage Hospital, Lond., 1877, and Paying Hospitals and Pay-Wards throughout the World, 1879 ; Parkes and F. de Chaumont, Reports on Hygiene in the Army Medical Reports; Id., Army Medical Regulations; Id., Naval Medical Regulations, and Annual Medical Reports, passim, Longmore, On Gun-Shot Injuries (for military hospitals), 1877 ; Reports of the State Board of Health, Massachusetts : Radcliffe, Report on the Manchester Royal Infirmary, and Report on the Norwich Infirmary ; Galton, Report on the Norwich Infirmary ; Roth and Lex, Handbuch der Milit. Gesundheitspflege, 1872-77; Langstaff, Hospital Hygiene, Lond.. 1872 ; Steele, Hospital Mortality, 1877; Tait, Hospital Mortality, 1877, Toilet, Sur les logements collectifs, Paris. 1878; "Account of Edinburgh Royal Infirmary," Scotsman, October 29, 1879 ; Reports on the New York Hospital (1877), Opening of Rhode Island Hospital (1808). New Pavilion Wards of Presbyterian Hospital, New York (1875), Pennsylvania Hospital (1879), Roosevelt Hospital (1879), St Luke's Hospital, New York (1860), Massachusetts General Hospital; Woodworth, Reports of U.S A. Marine Hospital Service, Hospitals, and Hospital Construction, and Report on the Hygiene of the U.S. Army, Washington, 1875; F. H. Brown, "Hospital Construction," in Buck's Hygiene and Public Health (1879). (F. DE C.)
Footnotes
[301-1] Liber ordinis Sancti Victoris Parisiensis, MS. cap. 40. Ducange's Glossary, s.v. "Infirmaria."
The above article was written by Francis Stephen Bennett François de Chaumont, M.D., F.R.S.; served in the Crimean War; Professor of Hygiene at the Army Medical School, Netley Hospital from 1863; author of Different Families of the Human Race and Hygiene in Civil and Military Life.
|